
The name Ruth Wakefield is not likely one that you recognize, but you most certainly know the invention she is credited for.
Ruth and her husband Kenneth owned a toll house in Whitman, Massachusetts in the 1930’s. Toll houses operated in the 1700-1800’s, serving not only as a building for which to collect tolls, but also as a haven for travelers to rest and enjoy a home-cooked meal. Ruth and her husband converted their toll house into a lodge, naming it the Toll House Inn.
True to the tradition of serving home-cooked food, Ruth baked for guests of the Inn. One of her favorite recipes to make was the Butter Drop Do cookie, and one day while she was making them, she decided to mix up the recipe by breaking a Nestlé chocolate bar into bits and adding them to the cookie. The delicious result was a cookie with soft, creamy chocolate morsels. Her recipe gained fame at the Inn and found its way into regional newspapers, exploding the sale of Nestlé chocolate bars.
Ruth’s innovation of tiny pieces of chocolate led to the creation of packages of chocolate morsels, or what we have come to call chocolate chips1.
Innovative ideas, like the chocolate chip, don’t always come from those in senior positions. Great ideas can—and should—come from those doing the work, like the baker. In behavioral healthcare this means that CEOs, directors, supervisors, and managers don’t possess all the solutions to the challenges their workforce faces. As leaders our charge is to empower direct care workers, peer support specialists, case managers, nurses, and other frontline workers to leverage their knowledge, experiences, and perspectives to challenge the status quo, make work easier, and serve people well.
To empower innovation on your team, consider the following:
Ruth was able to create the chocolate chip because she was directly involved in baking for the Toll House Inn. Because she was directly involved, she could see the challenge and solution to making Butter Drop Do cookies. Ruth was also empowered to try new ideas, free to explore cutting a chocolate bar into tiny pieces to see what would happen. And finally, Ruth had the time and resources available to set aside her other responsibilities and dedicate her attention to perfecting her recipe.
Direct involvement in the day-to-day work, empowerment, and the gift of time and resources are the recipe for innovation for frontline workers. Consider ways your program can bring innovative ideas to fruition through a thoughtful process, friendly competition, or the broadcasting and celebration of innovation.
*The invention of chocolate chips story was adapted from the History of Nestle Toll House.

Is your program required to undergo a program audit or quality site review? If so, it’s likely that just the term “audit ” creates an emotional reaction. Audits can seem like a disruptive annoyance, a “gotcha”, or a procrastinator’s nightmare, but it doesn’t have to be. Like most things, preparation is key. If you and your team are organized, understand the standards, have been keeping good records, and maintain audit readiness throughout the year, your experience may even be positive, and those auditors will be in and out in no time.
The American Society for Quality (ASQ) defines auditing as the on-site verification activity, such as inspection or examination, of a process or quality system, to ensure compliance to requirements. Auditing can also be done virtually or via a desk audit, where items are submitted for review to an auditor. Regardless of how you define auditing, everyone seems to dread an audit. Audits seem to raise a level of anxiety among people even if they believe they are following the “rules”. It does not seem to matter if the audit is internal or from an external entity, no one likes the “gotcha” experience and everyone wants to put their program in the best possible light.
Over the years,I have participated in many program audits. I have also conducted many audits and program reviews. Based on almost 30 years of experience, I have found the following activities not only prepare an organization for an audit but reduce the dread and anxiety that audits produce.
Get organized. Look at a calendar and determine how much prep time you have. Even with very short notice, you can successfully prepare for an audit. Obviously, the amount of time you have will dictate if this is an all-hands-on deck type of preparation or if you have time to thoughtfully divvy up tasks. Review all the information sent to you about what to expect from the audit and what will be required of you. Many times, audit notifications include specific documents that must be gathered, a calendar of activities or topics, individuals to be interviewed, etc. It is also a good idea to review previous audit reports including any corrective action plans that were implemented. Auditors will want to see evidence of those activities and ensure you have sustained improvement in those areas.
Review the standards.Take a good look at what will be reviewed. Standards may be outlined in a manual, in statute, in a contract, on a website, or provided in an auditing tool that will be used by the auditors. It is important to not only review the standards but understand their intent – “The spirit of the law”. By understanding the intent of the standard, you can identify the many areas one standard might involve. For example, a clinical program standard may require a signed consent on file. The intent of that consent is to inform the individual of the risks and benefits of the treatment prior to the provision of services. A signed consent does not meet the standard if it is signed after treatment begins or does not include a description of the risks and benefits of the treatment.
Identify your team.An audit should always be a team effort. It is a great way for staff to learn about the standards and how your organization’s policies and procedures are designed to meet the requirements. It is also a great way for staff to take ownership of their work. Lastly, participating in audit preparation can help individuals understand why certain things are in place. Have you ever had a staff person ask why a certain question is on an assessment or why you must do things a certain way? Most likely it is due to a standard or previous audit finding.
Collect evidence of compliance.Once you are familiar with the standards, begin collecting evidence that supports compliance with each requirement. Evidence may include policies and procedures, training records, clinical documentation, data, etc. Building this physical or electronic “proof box” of documentation is an essential part of being prepared and demonstrating your program’s compliance.
Conduct a gap analysis.Identify which areas you lack evidence of compliance, or areas where your evidence of compliance is not strong. It is always best to anticipate these areas and self-identify standards in advance where auditors may not find evidence of full compliance.
Develop a plan.If there is time, it is always best to attempt to obtain evidence of compliance or steps that are actively being taken towards meeting the standard. There are, however, some items where evidence just does not exist or is lacking. In those cases, the best way to address the lack of full compliance is to develop an improvement plan. An improvement plan can be implemented immediately and will demonstrate to the auditors that you are taking action to correct the issue. You may still be cited, but you will be proactive rather than reactive.
Conduct a mock audit. A mock audit is a great way to assess those areas that are not easily demonstrated through documentation. Mock audits can provide a realistic sense of policies and procedures in action and program staff’s knowledge and understanding of the standards. Mock audits can give you a true sense of what is or is not occurring in the program, offering the opportunity to interview staff, answer questions, and provide feedback.
Create an audit-ready culture.Creating the right culture is probably my most important tip. Coaching your program team to understand the standards, keep documentation up-to-date, and be “audit ready” year-round makes the actual audits less of a heavy lift and less anxiety-provoking. Audits can then be viewed as an opportunity for your program to shine!
We need innovative solutions to the mental health problems our communities are facing. How do we respond to increasing rates of depression and anxiety, the overuse of emergency rooms for mental health care, high rates of death by suicide and drug overdose, and budgets that never seem to cover what’s needed?
I’ve spent years facing these problems, yet I haven’t spent nearly as long considering the question that makes solving the problems possible: How does innovation happen?
I used to think innovation was the result of creative people’s spontaneous thinking. Imagine Alexander Graham Bell inventing the telephone by casually walking down the road and shouting, “Wait! Why walk to deliver this message on foot when I could transmit my voice through vibrations and current over wire!” Viola! Spontaneous innovation.
When I began reading the biographies of great innovators, however, I found they took a different approach. Leonardo Da Vinci transformed art not by obsessing about its current limitations, but by dialoguing with disciplines outside of art. Leonardo studied anatomy and the muscles that move lips to craft the world’s most intriguing smile. He talked with scientists about light, optics, and geometry to lead the Renaissance innovation of dimensionality in art. This was the spirit of the Renaissance, to learn broadly across disciplines and innovate through connection.
Four hundred years after Leonardo, Robert Oppenheimer led the Manhattan Project in pioneering the era-defining innovation of nuclear fission. He did this by the Renaissance method of finding connections in diverse ways of thinking. Growing up, Oppenheimer loved reading the classics in Greek and Latin, reflecting on French poetry, and admiring Dutch art. He continued this practice of absorbing diverse information and finding connections as a theoretical physicist and leader. In the daunting task of resolving the constant scientific arguments during the Manhattan Project, Oppenheimer was famous for listening to both sides, pointing out connections in the diverse ways of thinking, and thus illuminating a way forward.
In today’s age of unbelievable information and connection potential, the key ingredient now is the will to learn broadly across disciplines. For mental health innovation, what Renaissance connection is out there waiting for us? Here are a few promising directions I’ve seen:
Our communities need innovative solutions when facing mental health problems. Instead of waiting for a spontaneous innovation, we can listen to those outside of mental health and find the connections for the way forward. Let’s follow the Renaissance path, blazed by those who have changed the world.
Book References:
Leonardo Da Vinci by Walter Isaacson (2017).
American Prometheus: The Triumph and Tragedy of J. Robert Oppenheimer by Kai Bird and Martin Sherwin (2006).

Do you remember the moment you fell in love with your work?
For me, the most fulfilling experience of my career in
behavioral health care involved supporting and designing crisis
residential units1, or CRUs, across the state of Michigan. New
to the field as a macro social worker, I was privileged to be
considered a subject matter expert in CRUs by my peers. Soon
after, I was tasked with designing and opening a CRU in
Michigan’s Upper Peninsula, a project that brought me great
excitement and honor.
At the time, I knew little of the U.P., aside from its identity as a
winter wonderland far from home. I was committed to
designing and opening a CRU that met the needs of the U.P.
community, and I made it my mission to get to know the
extremely rural portion of my beloved state over several
months. This meant becoming a veritable dual citizen of the
upper and lower peninsulas of Michigan. Little did I know, this
dedication allowed me to avoid an incredibly prevalent
misstep in crisis services design and planning- plugging in a one-size-fits-all solution.
One-size-fits-all, or even one-size-fits-most, is a fallacy. A behavioral health crisis program or continuum
may appear to fit a community, but that does not mean it fits well. When the default is a one-size-fits-
all approach without considering the unique needs of a community, a mismatch or gap occurs and
complications can arise in our relationships where trust begins to erode, and doubt takes over.
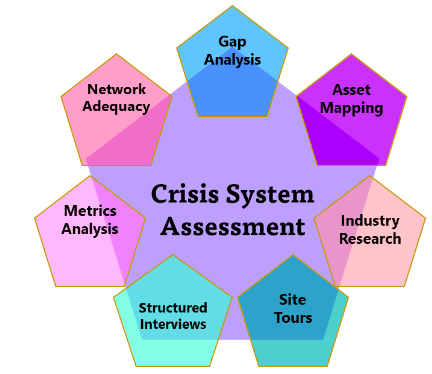
Crisis services are in the midst of a long-awaited and well-deserved spotlight. Thoughtful and sound research blended with the development of tools are advancing and expanding crisis system knowledge rapidly. While increasingly accessible tools inform the development of strong crisis services, no one tool is the golden goose. It would have been a grave mistake for me to assume that a program that found success serving Kent County, Michigan (population 658,046) would realize the same success serving all the Upper Peninsula (population 301,609 but 18 times larger in area). In population density alone, the differences paint a clear picture.
As you engage dialogue and planning for crisis service development and expansion in your community, consider what makes it unique. Do you live in a college or university town? Is your funding system complex and nuanced? Is the geographic location urban, suburban, rural, or frontier? Is there good access to public transportation, or have the tires of an Uber never touched the roads? Through thoughtful assessment and community engagement, the rightsized behavioral health crisis continuum can be developed in any community.
1 Crisis Residential Units are short-term behavioral health treatment programs in which individuals experiencing a behavioral health crisis receive person-centered care in a 24/7, homelike setting.

The Covid-19 pandemic has brought some much-needed attention to the role of direct care worker. Prior to the pandemic, a direct care worker was neither a well-known profession nor a well-appreciated one. The pandemic has highlighted how essential the direct care worker role is in providing care and brought attention to the workforce shortage of this profession.
What do direct care workers do?
Direct Care Workers (DCWs), also referred to as Direct Support Professionals, provide hands on care, supervision, and emotional support to individuals in nursing homes, mental health facilities, assisted living facilities and home-care settings. Many Direct Care Workers are required to administer medications as prescribed as well as monitor and report any changes in physical, mental, or emotional conditions. Direct care work is often provided 24 hours a day 7 days a week to America’s most vulnerable populations. DCWs implement care plans and provide the largest amount of direct contact with individuals in these settings.
Why is their work so important?
Direct care workers are responsible for providing assistance to those who struggle with activities of daily living such as mobility, bathing, cooking, cleaning, or other abilities many of us take for granted. Direct care workers spend most of their time directly with the patient. They are the eyes and ears of the professional staff who may only have moments in time with the patient. Direct care workers can provide vital information to their care team.
Direct care workers offer comfort to those struggling with a variety of issues including mental health issues. Direct care workers may often be the only individual a person speaks to on a regular basis or may be the only person available to share good news or bad. Much of what a direct care worker provides is not something that is prescribed – it is the care they offer that is often undervalued.
What does it take to be a direct care worker?
Some might say direct care work is a calling. Others see it as an opportunity to gain valuable experience in the healthcare industry. Regardless of the reason, there are six essential skills necessary to be successful as a direct care worker:
Empathy: The ability to relate to another’s experiences or conditions, such as joy, suffering, sadness, or anger
Patience: Encouraging growth while moving at the pace of the person served
Compassion: Sympathetic awareness of the distress of the person served and a desire to alleviate it
Adaptability: Capability to adapt to new, different, and changing situations.
Reliability: Possessing the quality of being trustworthy or of performing consistently well.
Attentiveness: Attending to the comfort, well-being or wishes of the person served.
What are the benefits of being a direct care worker?
Although the work can be challenging there are many benefits to being a direct care worker. Those benefits include:
Rewarding and meaningful work
Ability to express and use inherent skills
Flexible hours for those who need a non-traditional schedule
The opportunity to grow interpersonal skills
There is a high need/demand for this type of work
What has impacted the direct care worker shortage?
There are many factors that have led to individuals leaving the direct care worker profession as well as preventing individuals from entering the direct care worker profession. Some of these factors include low wages or lack of guaranteed hours. Many agencies that employ direct care workers have limited employee benefits such as health insurance coverage, sick leave, or retirement benefits. The environments in which direct care workers are employed have high levels of physical and emotional stress and lack supervision or management support. The stress experienced by direct care workers is often due to inadequate training. Individuals employed as direct care workers are often not respected for their knowledge and skills and are not provided professional growth opportunities.
What is the future of the Direct Care Worker workforce?
The need for direct care workers is expected to increase over the next 10 years due to a growing population that needs their support. While the need increases, the vacancy rate for direct care workers is also expected to increase. The future of the direct care workers workforce will require creative recruitment and retention strategies. Without a focus on developing this important workforce, our most vulnerable will not have the assistance they need or quality of care they deserve.
Americans, I. o. (2008, May). Retooling for an Aging America: Building the Health Care Workforce.
Retrieved from Washington (DC): National Academies Press (US):
https://www.ncbi.nlm.nih.gov/books/NBK215393/
Healthcare, O. S. (2019, October 8).What Makes a Successful DSP? Retrieved from Open Systems
Healthcare: https://opensystemshealthcare.com/what-makes-a-successful-dsp/
Kezia Scales, P. (2021, June). It is Time to Resolve the Direct Care Workforce Crisis in Long-Term Care.
Retrieved from The Gerontologist, Volume 61, Issue 4, pages 497-504:
https://doi.org/10.1093/geront/gnaa116
Taylor, J. (2022, April 27). Direct-Care Workers share their experiences amind the critical shortage.
Retrieved from Spartan News Room:
https://news.jrn.msu.edu/2022/04/direct-care-workers-share-their-experiences-amid-the-critical-shortage/
Vizzini, N. (2018, February 15). 5 Reasons to Become a Direct Care Worker.
Retrieved from Horizon Staffing Solutions:
https://www.horizonstaffingsolutions.com/reasons-to-become-a-direct-care-worker

Several years ago, I watched a 60 Minutes interview with a security guard at an airport who recalled one of the worst days of his career. He had unknowingly allowed a small group of conniving conspirators to pass his purview without stopping or interrogating them. While he didn’t know it at the time, this oversight would have devastating global consequences.
The date was September 11, 2001.
While the security guard was one of dozens of airport and airline employees that day who would allow global terrorists to pass before their eyes, the disturbing fact remained: an avoidable tragedy had transpired, leaving these people and millions of others feeling hopeless and helpless as thousands lost their lives. While there is nothing that can be done to change that fateful day, nearly every person hopes to find a way to be truly helpful in preventing or responding to a tragedy, especially those that impact the loss of life.
Unlike 9/11, the warning signs of COVID-19 are now blindingly clear to many who are in a position to help.
As doctors, elected officials, scientists, behavioral health professionals, and armchair epidemiologists offer their guidance, the United States is responding to the healthcare crisis at hand while preparing for the healthcare tsunami that is about to unfold, the latter of which will have epic consequences on our healthcare infrastructure, mortality rates, and social wellbeing if we are not adequately prepared and responding. The world is changing before our very eyes, and we are called to see clearly and act intentionally and thoughtfully.
As a behavioral health consultant, I spend much of my time researching how communities respond to people experiencing psychiatric emergencies. Historically, people in a mental health crisis have accessed care through services designed for people with medical emergencies—namely, 911, emergency medical services (EMS), and hospital emergency departments. Progressive communities have boldly embedded services like suicide prevention hotlines, mobile crisis teams, psychiatric urgent care centers, and residential crisis stabilization programs to provide dedicated attention and focused responses to psychiatric emergencies. Some of these services also have the added benefit of diverting people from psychiatric hospitalization in instances where it is not necessary. These crisis services have reported tremendous results, with each alternative service option typically resolving the crisis without having to access the next more intensive level of care in 70-85% of the cases.
Amid the turmoil of the COVID-19 pandemic, it is imperative that these crisis services remain intact to address both the usual behavioral health emergencies as well as those created or exacerbated by anxiety, isolation, unemployment, limited access to critical resources, increased substance use, and other unintended consequences of social distancing and shelter-at-home declarations.
While the future is never completely predictable, it is possible to see problems unfolding and to infer their effects based on our knowledge of the system’s current issues. Here is a summary of current issues developing within the behavioral health safety net with a corresponding set of proposed solutions to keep us from the worst-case scenarios we all dread—untreated mental health crises and increased deaths of despair, such as suicide or overdose.
PROBLEM:
Crisis Call Centers are losing capacity due to staffing and technology challenges. There are approximately 700 crisis call centers in the United States designed to support people experiencing emotional distress, extreme anxiety, suicidal thoughts, and other distressing mental states. Smaller call centers are often staffed with a student or volunteer workforce with office-based phone lines. Several confounding variables emerging in this national crisis are limiting their ability to function, including limited budgets, reduced workforce accessibility, and undeveloped remote technology. Fewer staff answering phones means longer wait times and more people hanging up without talking to someone, resulting in less ability to resolve the crisis and potentially divert someone from a higher level of care. In addition, well-intended actions to socially distance “non-essential” staff are having negative impacts: call center workers are willing to work remotely but are unable to do so, putting them at risk for becoming unemployed.
SOLUTIONS:
Re-allocate resources to maintain crisis call center capacity. In organizations where outpatient services have been closed or moved to telehealth options, redeploy crisis workers to the phone lines to maintain necessary capacity. Coordinate with information technology (IT) staff and vendors that have successfully navigated this transition with other call center-based service providers to transition people to a mobile platform as quickly as possible.
Train and support staff to assure a smooth transition to telehealth functioning. While crisis call center employees are comfortable with telephonic-based service environment, reassigned mobile crisis workers or outpatient clinicians may not seamlessly transfer their skill sets to the phone lines. Assure that staff are receiving regular supervision and staying attuned to their emotional reaction to their work as well as the ongoing pandemic. Reinforce professional boundaries that balance the tension of building rapport with serving the person in crisis without allowing staff’s unmet emotional needs to interfere with crisis resolution.
PROBLEM:
Health plans have fewer mental health resources to rely on, leaving members in crisis without adequate treatment. Nearly all outpatient services have been moved to telehealth with corresponding billable services where available. Considering that most hospitals have more than 16 beds, some psychiatric hospitals are decreasing their census capacity in an effort to practice social distancing and comply with state and federal regulations limiting groups of 10 or more. The combination of these two factors may leave health plans scrambling for solutions for their members in crisis.
SOLUTION:
Health plans should pursue case rate agreements with local crisis service providers to maintain network adequacy and proactively address psychiatric crises. Mobile crisis teams, 23-hour crisis stabilization facilities, and crisis residential services are viable alternatives to ED utilization and psychiatric hospitalization when there are no other major underlying medical issues. In some cases, these alternative services can also treat co-morbid medical and/or substance use conditions. While most commercial health plans have been slow to contract for these types of crisis services, and Medicare does not currently cover crisis services, the impetus has never been greater to broaden the service array and mitigate risk for their members. At some point, all payers will be seeking sources of refuge for their members with psychiatric emergencies that keeps them from imminent exposure to the virus whenever possible. Providers can respond to the call with a bevy of research and data to support the efficacy of their services.
PROBLEM:
Crisis providers are working without one of their most precious resources—their physical presence. Crisis call centers notwithstanding, moving from in-person services to telehealth is like being forced to use your weak hand to write a two-page essay: you can adapt, but it certainly doesn’t feel natural. Without having the advantage of observing the environment, the entire body for nonverbals, peripheral social interaction, and other cues, it can be difficult for clinicians to effectively do their job.
SOLUTION:
Double down on wellness, maintenance, and crisis postvention check-ins. Maintaining good rapport and keen insights on wellness and symptoms requires frequent connection. Communities that have already built crisis postvention resources as part of the best practices identified by Zero Suicide are well-positioned to expand these resources to as many clients as possible, starting with high-risk and post-crisis individuals. Identify the critical, basic skill set required for telehealth check-in’s and follow up and engage as many of your staff as possible to pick up the phone or tablet and reach out. Symptom rating scales can also be useful to monitor mood and symptoms. Lastly, provide training and ongoing supervision to assure competency in delivering these services and monitoring staff wellness. Organizations like the National Suicide Prevention Lifeline have developed resources for crisis providers transitioning their workforce to remote settings.
PROBLEM:
Crisis providers may be excluded from conversations about “essential services” to remain open, limiting their ability to be helpful. Peer respite homes are temporary sanctuaries for people experiencing emotional distress or crisis who prefer to receive support in a non-medical environment. Approximately 75 peer respite homes exist in the United States, but many have closed temporarily in the past week at the discretion of their funders while increasing their warmline (i.e. non-crisis line) capacity, in some cases to 24/7 operation. Other crisis residential providers are uncertain of their fate as census numbers have fluctuated over the past few weeks and their access to personal protective equipment (PPE) is limited in the event a staff or client contracts the virus.
SOLUTIONS:
Include crisis providers in community decisions about essential services as the needed adaptability to solve critical system deficiencies. For decades, crisis providers have been the business of finding ways to say “yes” and offering adaptable solutions to community problems. Crisis residential providers are already adjusting to community need by extending the length of stay in their programs to mitigate COVID-19 exposure and setting up tents outside of their facility for health screenings according to CDC guidelines. Some providers are redeploying outpatient practitioners to crisis services to manage the projected surge in treatment need. Public health and disaster preparedness planners would be well-served to invite behavioral health crisis providers to the table to improve planning and response to local, regional, or national crises.
Establish and reinforce a strong pipeline of communication between mental health authorities, providers, and persons served. While many of us are plugged into the 24-hour news cycle, people with less access to resources and more environmental stressors may not be attuned to the latest preventative measures and treatment protocols. When coupled with increased isolation or anxiety from perceived or actualized fears of contracting the virus, it is even more imperative that persons in crisis receive regular updates on how their treatment is being impacted and what providers are doing to promote client health and safety.
PROBLEM:
Mobile Crisis Teams have been temporarily displaced as their work is typically done face-to-face. While new telehealth laws make it easier to provide these services remotely, most mobile crisis teams are not designed to provide care in this way and may not have the HIPPAA-compliant technology to adapt in this circumstance (although some states are temporarily waiving the HIPAA-compliant requirement at this time).
SOLUTION:
Coordinate telehealth assessments between mobile crisis teams and EMS, Law Enforcement, and Emergency Departments. Keeping assessment and disposition time short is critical to maintaining capacity for the expected influx of medical and psychiatric emergencies. If first responders can use HIPAA-compliant assessment software on a secured mobile device when dispatched, they can connect the person in crisis with the proper support in an efficient and flexible manner.
I hope that, in the midst of the COVID-19 crisis, we experience our finest hours of coming together to showcase the very best that we can be as health care professionals, as community partners, and as compassionate humans. With careful and conscientious planning and response, we can minimize the tragedies that this pandemic could incur, finding ourselves stronger and more resilient on the other side of this epic, civilization-wide trial.
If security measures had not increased following 9/11, we would consider the Federal Aviation Administration negligent for not working to prevent future tragedies. We face a similar opportunity today as the lessons learned by other infected countries color our prevention and treatment responses.
Years from now, I hope the 60 Minutes story that profiles behavioral health services during COVID-19 is one that we can be proud of, knowing that we were the most helpful in the greatest time of need.
The photo credit is: Photo by Braden Hopkins on Unsplash

Supporting a Workforce Experiencing Change Fatigue
Behavioral health organizations are no strangers to change. Evolving procedures, new documentation practices, technology upgrades, and staff
turnover are par for the course. However, the pandemic has brought with it a level of chronic change seldom before experienced and exceedingly difficult to adapt to. Employees have been asked to acclimate to changes associated with remote work, new business models, organizational restructuring, and countless iterations of Covid-19-related protocols. “Business as usual” has constantly adjusted.
As humans, we inherently need structure, routine, and reliability. Change, at the pace, it has occurred since the pandemic began, has disrupted these basic needs. According to research from Gartner, employees’ ability to cope with change is half what it was pre-pandemic i. This type of fatigue, known as change fatigue, is characterized by an organizational culture of stress, confusion, apathy, and resistance in the face of change due to multiple concurrent changes or a history of failed change attempts. Today’s behavioral health workforce faces change fatigue on top of existing compassion fatigue and burnout.
It is important to recognize, respond to, and work to prevent change fatigue. To spot it in employees, look for these signs and symptoms:
Frequent, loud complaints
Indifference (or even disengagement)
Visible tiredness
Anxiety
Push-back
Prevailing negativity
Skepticism about change success
Loss of focus
Eroded morale
Absenteeism
The complex change occurring in behavioral health organizations today requires strategic change management. The timeless Managing Complex Change Model, published by Timothy Knoster, asserts that to successfully implement change, you must have vision, skills, incentives, resources, and an action plan. ii Missing any of these key pieces can lead to the signs and symptoms of change fatigue listed above.
Behavioral health organizations must confront change fatigue in order to
recoup staff engagement and produce desired outcomes for the people they serve. There is no quick fix for change fatigue but utilizing the strategies below can help refuel teams who are running on empty and equip them for more change ahead.
Demonstrate purpose and meaning in the work – According to Gallup, a key driver of employee engagement is purpose in the work.iii Find ways to remind employees why what they are doing every day is important.
Build trust and team cohesion – Prove that you have employees’ interests in mind and do what you say you are going to do. Nurture connection among the team and foster commitment to the common goal of your program.
Cultivate caring managers who are effective at coaching employees
to the next level – The manager alone accounts for 70% of the variance in team engagement. iv Invest in their leadership and relationship development skills.
Communicate early and continuously – Bring employees into the change journey early on so they can mentally prepare. Update them as the change progresses. Keep a pulse-check on the impact as time goes on and offer support as the reality of the change sets in.
Engage leaders and teams (at all levels) most affected by the change in the planning and implementation – Individuals support what they create. Include them in shaping the change experience.
Stage activities to control the pace of change – Few changes are debatable; however, timing is frequently adaptable. Space change activities out to a manageable tempo.
Characterize the result of each change – Without an understanding of the conclusion, the full extent of a change cannot be comprehended. Loopback around with your team about the change and be transparent about the outcomes and lessons learned.
Change is inevitable. It can be met with excitement, apprehension, or both. For a workforce that is vulnerable, change must be introduced and executed thoughtfully. Assess the team’s readiness for change, communicate throughout the process, involve them, and share the end result.
The photo credit is: Photo by Elisa Ventur on Unsplash
i Baker, Mary (2020). How to Reduce the Risk of Employee Change Fatigue. Change fatigue is rising; first tackle small everyday changes (gartner.com)
ii Knoster, T., Villa, R., & Thousand, J. (2000). A framework for thinking about systems change. Restructuring for caring and effective education: Piecing the puzzle together, 93-128.
iii The Gallup Organization. (2020). What Is Employee Engagement and How Do You Improve It? Gallup,
Inc. https://www.gallup.com/workplace/285674/improve-employee-engagement-workplace.aspx
ivThe Gallup Organization. (2020). What Is Employee Engagement and How Do You Improve It? Gallup, Inc. https://www.gallup.com/workplace/285674/improve-employee-engagement-workplace.aspx
A friend recently shared with me her experience of training staff at a behavioral health center in trauma-informed care. She asked for participants to share an example of when their work had triggered their own trauma response and her question was met with a gripping silence as a blanket of tension pressed heavily on the room. It was clear participants did not want to share or didn’t feel safe enough to share. Rather than simply moving on or providing a cookie cutter example, she took a risk. She chose to be vulnerable and share her experience of being triggered during a family session due to trauma she experienced in her marriage. Her intentional choice to be vulnerable and share something personal opened a doorway for others. The feeling in the room shifted and a participant was then able to share their own trauma response experience.
Another friend participated in a national behavioral health leadership program and returned from one of the conferences energized and passionate about the power of vulnerability in leadership. So, I did what any person like me would do when something piques my interest: I googled it. I spent a few hours reviewing articles on trauma-informed systems of care and the power of vulnerability. I also reflected upon my time working at two behavioral health organizations as staff learned to adopt a trauma-informed culture.
These two incidents occurring so closely together made me pause and consider how a leader’s level of vulnerability might be correlated with the degree to which that organization’s culture is trauma informed. The basic characteristics of a Trauma Informed System of Care (TISC) include safety, trustworthiness, choice, collaboration, and empowerment. To become a TISC, an organization must examine multiple aspects of the system, including the physical environment, clinical assessment, and interventions, staff relationships and morale, organizational communication, response to secondary trauma, etc. It is a culture, not a set of services or interventions. Leaders must learn to be vulnerable if there is any hope for their organizations to truly adopt this trauma-informed culture. This culture must include everyone, from clerical staff to the cleaning crew, to clinicians and perhaps most importantly (and often overlooked), leadership.
Regardless of where your organization is on the journey to becoming a TISC, as a leader in your organization, challenge yourself to explore how vulnerable your team is willing to be, and your own reactions to vulnerability. Do you avoid it? Do you see vulnerability as a weakness? Do you become anxious or tense at the thought of sharing personal experiences with your co-workers? Do you feel your co-workers need to “suck it up” and not be so “needy”? Do you view co-workers as overly dramatic and attention seeking? Do you feel disconnected from others at your workplace? Do you rationalize your emotional distance by telling yourself that you shouldn’t have meaningful connections with others at work or that you need to maintain an image of strength? Do you find yourself fighting back when someone criticizes you or your decision?
Or, do you embrace your vulnerability? Brene Brown and Myric Polhemus both discuss the critical importance of connecting deeply with the people with whom you work. A leader must be vulnerable in order to truly connect with her staff. Are you self-aware? Do you reveal your thoughts and feelings to others, even when doing so makes you feel emotionally at risk? Are you open to considering you made a mistake? Do you admit it when you’re wrong? Do you approach your imperfections with humor and grace? Do you ask clarifying questions to better understand your co-workers, especially when you disagree with them? Do you truly listen to their perception of events and allow this to alter your perceptions?
By opening yourself up to be vulnerable, your employees will follow your example, and find motivation from a genuine interest to serve (relationship power), rather than feeling coerced (role power). By fostering deep and meaningful connections with your staff, they will learn to feel safe, a fundamental requirement of a TISC. I have observed that when staff on my team felt secure (in their position, in the organization) they were more likely to provide needed feedback to the organization and to be more innovative. Leaders work tirelessly to ensure that those served by the organization feel safe, supported and that the systems of care do not re-traumatize them. As leaders, we should settle for no less for our staff.

Buzz words.
We seem to have a love/hate relationship with them. Even if we try not to, we find ourselves using them in meetings or in discussion with co-workers. In healthcare, the “Triple Aim” is one of these.
The concept is great: Improving the patient experience of care AND improving the health of populations AND reducing the per capita cost of health care.
“Triple Aim” has definitely become “a buzz” within the behavioral health community over the past few years. Many behavioral health organizations have included it in their mission, vision or strategic plan. These important tools identify the direction of the organization.
But if the focus on the Triple Aim never escapes the C-Suite (CEO, COO, CFO, etc.), there is risk that it will not become embedded within the workplace culture and actually impact workflow, outcomes, and ultimately, the people whose lives it could benefit most.
It is far easier to discuss buzz words than actually adapt our business to reflect a new reality. To adapt to a new environment or the presence of a new variable is challenging. It’s also necessary. Adaptation can take years but ultimately can determine your organization’s survival.
Biologists are very familiar with this concept. Rosemary and Peter Grant are two researchers who spent almost 30 years researching the finch population on two small islands, Daphne Major and Genovesa, in the Galápagos archipelago, Ecuador. They found that there was a difference in the size of the ground finches’ bills between islands. The size of the bills was conditional upon which other finch species were present. To survive and thrive, these animals had to adapt. I propose that program managers within your organization need to be like those finches.
Program managers within behavioral health organizations have a great opportunity to use the Triple Aim as a foundation for program evaluation. My experience has been that a program manager’s time is often consumed by meetings, staff supervision, reviewing staff documentation, updating policy and procedures, preparing for audits and accreditation surveys, as well as the ever popular and time-consuming HR problems. With all these demands, it is no surprise that it can be very challenging to actually engage in meaningful program evaluation and identify any areas in which the team may need to adapt.
If you are leading a behavioral health program, such home based therapy or case management, the Triple Aim framework can be used to evaluate and improve the program.
Does your team utilize patient satisfaction measures? Are they meaningful or a survey that staff pass out once a year that most patients throw away? How are your staff collecting patient report of satisfaction on an ongoing basis? Do they simply check “satisfied” in the progress note if the patient didn’t seem upset about their services that day? Or do they have meaningful discussion with persons served about how services are helping them and any changes that need to be made? How do you measure quality of your services? Do you use fidelity measures for best practices? Once patient satisfaction and quality metrics are measured, do you share this information with staff? With persons served?
This one can seem pretty overwhelming. Behavioral health clinicians work very hard to keep those they serve out of jail, inpatient units, etc. Improving their health may feel like an impossible task — but it’s not! Start small, pick one population you want to target, such as children taking atypical antipsychotics or adults with diabetes and depression. Define clear goals and measures. Work closely with your information specialists and analysts to identify a way to collect data and track your outcomes. Implement Plan, Do, Study, Act (PDSA) cycles to improve care. Research shows that persons with severe and persistent mental illness die, on average, 25 years younger than the general population, often due to treatable conditions*. Therefore, it is critical that we adapt the care that we provide to be more integrated, focusing on overall health.
In some behavioral health organizations, program managers may think “How am I supposed to impact cost? Isn’t that the finance department’s job?” If you feel out of the loop regarding the cost of your program:
These activities only focus on the cost of your team’s services. That’s a good start. But to impact per capita cost, you have to look at all health care costs. This is a significant challenge.
Even though we now have growing access to encounter data and various data analytic software packages, many do not include cost data. There are some creative efforts at the local level to engage in dialogue with other health care providers via regional health improvement councils. What’s needed are data sharing agreements or releases of information to gain patient consent so that protected health information data can be shared.
Dialogue with community providers can help you identify ways to reduce the cost for specific populations. You could also try contacting a player, such as a Medicaid HMO, that provides coverage for a large portion of the population you are addressing. They may be willing to work with you on a pilot project and would be able to track the overall cost of your participants (for which they provide coverage).
In the ever-changing landscape of healthcare reform, it is increasingly critical for behavioral health providers to be competitive within the larger health care market. Now more than ever, we need to be able to demonstrate effective outcomes (evidenced by data!), competitive costs, and high patient satisfaction.
We encourage you to use team/individual goal setting and process improvement teams as an opportunity to integrate Triple Aim principles into your workflow and agency culture. This will help you to flourish in the era of integrated, value-based care. Implementing Triple Aim goals at the program level and monitoring progress with data will help ensure your success.
* For additional information please see Morbidity and Mortality in People with Serious Mental Illness,” published in October 2006 by the National Association of State Mental Health Program Directors (NASMHPD) Medical Directors Council (http://www.nasmhpd.org/) and an earlier report by the Center for Mental Health Services of the Substance Abuse and Mental Health Services Administration (SAMHSA), Sixteen State Study on Mental Health Performance Measures. Rockville, MD: DHHS Publication No (SMA) 03-3835; 2003).

In behavioral health treatment, the pendulum of personal and professional experience has slowly swung from side to side for the past century. From Alcoholics Anonymous to the advent of Vet Centers for returning Vietnam veterans, peers have exemplified the power of empathy by supporting one another through shared life events. Their firsthand knowledge helps to bridge the chasm of fear that clients carry that they will not be truly understood.
While peer support has grown and evolved, so, too, have the clinical professions and their effectiveness. Identifying and implementing best practices in therapeutic settings have helped change the face of clinical services, from a nebulous, undefined journey through the subconscious to a meaningful service that delivers results.
As recently as 5 years ago, graduate training programs in fields such as psychology, counseling, and social work did not give substantial attention to peer support or sharing personal experiences as an effective treatment tool, instead advocating an approach that all but extinguished self-disclosure in a therapeutic setting due to fears of transference and crossing professional boundaries.
Empirical studies that validated the tools and methods of clinical professionals are now affirming the effectiveness of peer supports in treatment settings, demonstrating similar outcomes to their more educated constituents. In the last 10 years, many states have formalized the training and certification process for peer support specialists, bringing a level of credibility to their work that has not previously been seen. To make matters more complex, clinical professionals and peer supports are now working side-by-side in recovery-oriented systems of care, forcing both parties to recognize one another’s skills while working together to provide effective treatment.
In a healthy recovery-oriented treatment environment, clinicians and peer supports would complement one another in doing what is most helpful for the client: supporting their recovery. With all of the changes that have occurred in both fields, what will the next 100 years bring?



